Don't confuse the "Prevention Theory" of raising your 25D level with reality
Why doesn't intervention work?

This is what you are up against. FORTY PLUS Doctors working together all following association based 25D testing. Grassroots
They create a world where your “low” 25D level during your lifetime determines if you get cancer or some other disease later in life. Woulda, coulda, shoulda Vitamin I always say. The founder had breast cancer and just knew she had failed and now with the other Doctors, they will make sure everyone MAINTAINS high levels of only TWO of at least 15 unique 25D molecules. Not including the ones the body makes when sick or children make when supplemented mind you. Nope. Just the 25D that would be created by the sun, food or supplements. You know, the throughput of the PILLS that are sold. Mostly made by Hoffman LaRoche. They make tests and own most the labs too.
Think about their position, these Doctors at Grassroots
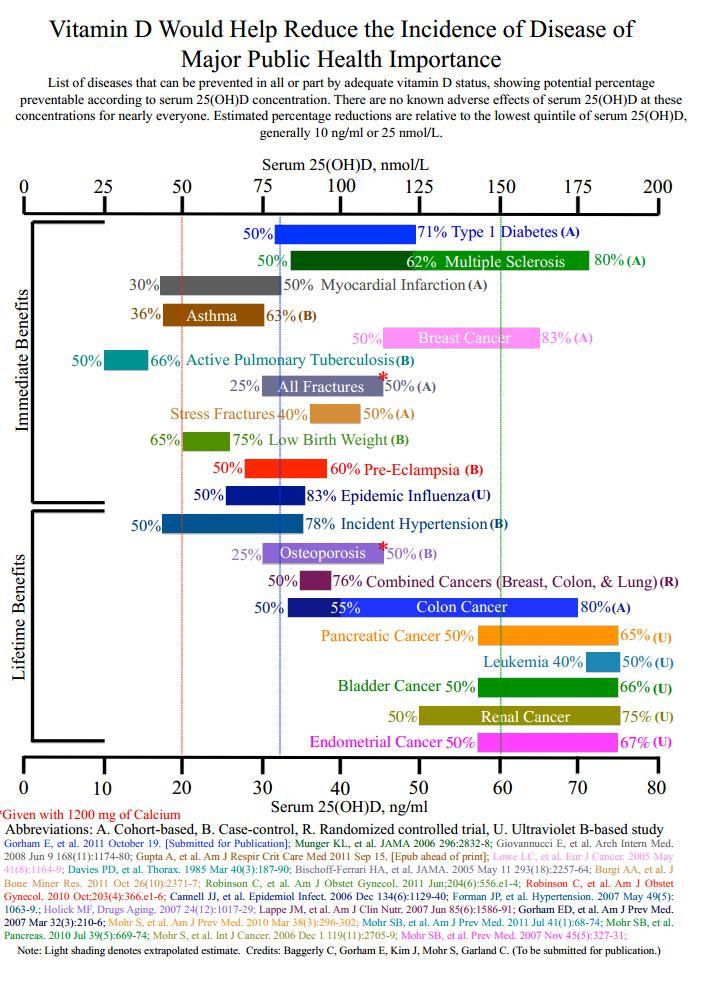
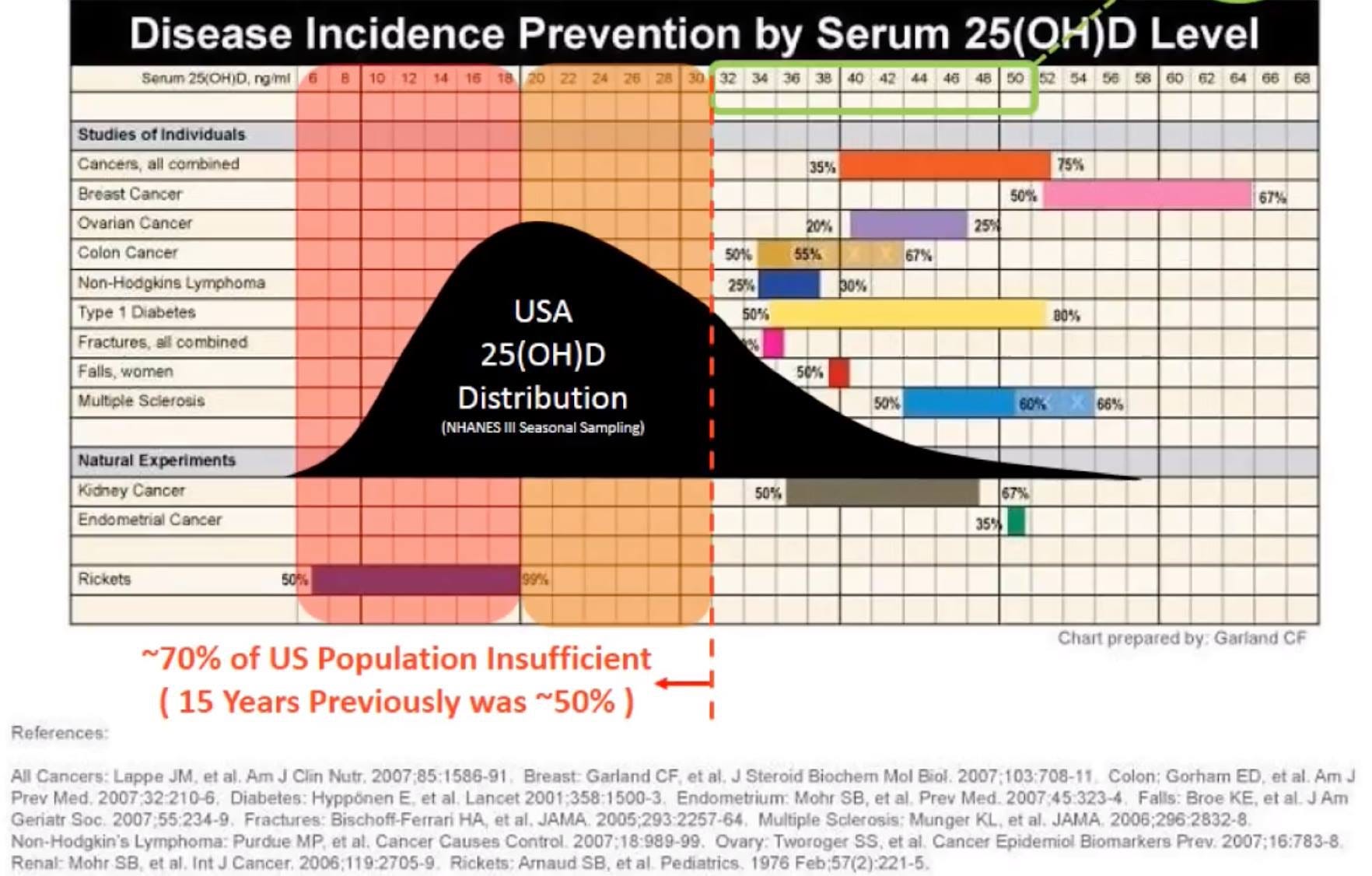
Disease Incidence Prevention by Serum 25(OH)D level. There aren’t publications like this with Vitamin A at the top or any other important molecule. Only D can get published based upon correlation equals causation summation. It’s over. It was your silly liver and your low 25D. 🤷🏼♂️
So instead of having “low” 25D during your lifetime you will stay above the natural limit the body seems to observe, 60ng/150nmol.
They are telling you by doing this you will avoid those diseases.
The sad truth is no one will be looking for hypercalcemia CORRECTLY, you may be allowed to have your kidneys remove excess calcium for years before the serum will show hypercalcemia. Try to find THAT study. Go for it. How long and how much D is necessary to spill over into serum from urine? It’s not gonna exist silly rabbit.
From top Dog at Vitamin D Council: "The first sign of vitamin D toxicity is Hypercalciuria (excess calcium in the urine), not hypercalcemia (excess calcium in the blood)." NOT the blood tests everyone is using.
You will Exhaust telomeres. You can only build so much bone in a lifetime.
Abstract
Caloric restriction prolongs life span. Calcium restriction may preserve bone health. In osteoporosis, bone mineral density (BMD) has significantly decreased, due to a lack of osteoblast bone formation. Traditional osteoporosis prevention is aimed at maximizing BMD, but the lifetime effects of continuously maintaining a high BMD on eventual bone health in old age, have not been studied. Strikingly, in countries with a high mean BMD, fracture rates in the elderly are significantly higher than in countries with a low mean BMD. Studies show that this is not based on genetic differences. Also, in primary hyperparathyroidism, on the brink of osteoporosis, BMD levels may be significantly higher than normal. Maybe, BMD does not represent long term bone health, but merely momentary bone strength. And maybe, maintaining a high BMD might actually wear out bone health. Since osteoporosis particularly occurs in the elderly, and because in osteoporotic bone less osteoblasts are available, the underlying process may have to do with ageing of osteoblastic cells. In healthy subjects, osteoblastic bone cells respond to the influx of calcium by composing a matrix upon which calcium precipitates. In the process of creating this matrix, 50-70% of the involved osteoblasts die. The greater the influx of calcium, the greater osteoblast activity, and the greater osteoblast apoptosis rate. An increased osteoblast apoptosis rate leads to a decrease in the age-related osteoblast replicative capacity (ARORC). In comparison to healthy bone, in osteoporotic bone the decrease in the replicative capacity of osteoblastic cells is greater. Due to the eventual resulting lack of osteoblast activity, micro-fractures cannot be repaired. Continuously maintaining a high BMD comes with continuously high bone remodeling rates, which regionally exhaust the ARORC, eventually leading to irreparable microfractures. Regarding long time influences on bone health, adequate estrogen levels are known to be protective against osteoporosis. This is generally attributed to its inhibiting influence on osteoclast activity. Instead, its net effects on osteoblast metabolism may be the key to osteoporosis prevention. Adequate estrogen levels inhibit osteoblast activity, calcium apposition and osteoblast apoptosis rate, preserving the ARORC.
CONCLUSION: Regarding osteoporosis prevention, ARORC better than BMD represents bone health. Regarding ARORC, adequate estrogen levels are protective, opposing the similar effects of hyperparathyroidism and a high calcium diet. Tests need to be performed in mice to assess the lifetime effects of a high versus a low calcium diet, on eventual bone fracture toughness.
https://www.ncbi.nlm.nih.gov/m/pubmed/15949902/
They are admitting it’s a woulda, shoulda, coulda situation too because they can’t link any successful disease intervention papers. NONE exist.
So, the association-based pseudoscience drives a religion type movement that is supported NOT by papers but by the self-fulfilling prophecy carried out by the church’s members via steroid and placebo effect that makes them true believers.
Is Grassroots full of true believers? One would hope so. Now let’s give a breast cancer survivor, just wanting to do good and help others avoid what happened to her, the benefit of the doubt and ask ourselves the following question. (From my perspective)
Am I such an AMAZING armchair researcher that I was able to find some of the RIGHT “Vitamin D” molecules that work on cancer in the HERE AND NOW, but these 40 plus Doctors, working together to try to keep folks from GETTING CANCER, didn’t or couldn’t?? PLEASE.
Now ask yourself what is their pathogenesis model, how does the 25D prevent the cancer or disease. What’s it do? What does it become? The MOST BASIC PHUCKING questions folks. In a FORTIFIED SOCIETY! Have these questions been answered NINETY-TWO years after it began? No. That doesn’t make any CENTS. Don’t be such a FOOL. CONSUME. DESTROY your body. Join the church of 25D. Everyone’s welcome. Everybody’s ”deficient” after all. Anyone can be healed, or become a Preacher or a Nun. The person that sells you your D will never discriminate. Come one, come all. Bring us your masses. Join our Mass.
Oh, you have a VDR SNP. Poor dear. You belong here. Partake.
Studies I can find but the Grassroots Doctors can’t.
Let’s start with ergosterol that didn’t receive UVB. Mushrooms.
Ergosterol acted upon by a CYP enzyme rather than UVB:
17alpha,24-Dihydroxyergosterol inhibited cell proliferation of HaCaT keratinocytes and melanoma cells.
https://www.cell.com/cell-chemical-biology/fulltext/S1074-5521(05)00199-7
Now let’s look at the D2 potential post UVB exposure.
People quite often say that D2 is not effective at raising peoples 25D level.
First you have to realize that vitamin D2 will always be D2 and vitamin D3 will always be D3. Each one makes unique analogues. They also have different affinity to the carriers and the receptors as well as differences in half-life.
In this case D2 went to the 20(OH)D2 pathway. The body decides, you can’t control this. So this would result in it looking like D2 is ineffective in raising 25D. It’s quite effective in raising 20D!!!!
Here are two examples of unique D2 analogs that would be created and not detected in current testing. Please notice that these molecules don’t lead to calcemic effects and as such would have been historically labeled inert. Clearly they are NOT inert.
“20-Hydroxyvitamin D2 is a noncalcemic analog of vitamin D with potent antiproliferative and prodifferentiation activities in normal and malignant cells”
“20-hydroxyvitamin D(2) [20(OH)D(2)] inhibits DNA synthesis in epidermal keratinocytes, melanocytes, and melanoma cells in a dose- and time-dependent manner. This inhibition is dependent on cell type, with keratinocytes and melanoma cells being more sensitive than normal melanocytes. The antiproliferative activity of 20(OH)D(2) is similar to that of 1,25(OH)(2)D(3) and of newly synthesized 1,20(OH)(2)D(2) but significantly higher than that of 25(OH)D(3). 20(OH)D(2) also displays tumorostatic effects. In keratinocytes 20(OH)D(2) inhibits expression of cyclins and stimulates involucrin expression. It also stimulates CYP24 expression, however, to a significantly lower degree than that by 1,25(OH)(2)D(3) or 25(OH)D(3). 20(OH)D(2) is a poor substrate for CYP27B1 with overall catalytic efficiency being 24- and 41-fold lower than for 25(OH)D(3) with the mouse and human enzymes, respectively. No conversion of 20(OH)D(2) to 1,20(OH)(2)D(2) was detected in intact HaCaT keratinocytes. 20(OH)D(2) also demonstrates anti-leukemic activity but with lower potency than 1,25(OH)(2)D(3). The phenotypic effects of 20(OH)D(2) are mediated through interaction with the vitamin D receptor (VDR) as documented by attenuation of cell proliferation after silencing of VDR, by enhancement of the inhibitory effect through stable overexpression of VDR and by the demonstration that 20(OH)D(2) induces time-dependent translocation of VDR from the cytoplasm to the nucleus at a comparable rate to that for 1,25(OH)(2)D(3). In vivo tests show that while 1,25(OH)(2)D(3) at doses as low as 0.8 μg/kg induces calcium deposits in the kidney and heart, 20(OH)D(2) is devoid of such activity even at doses as high as 4 μg/kg. Silencing of CY27B1 in human keratinocytes showed that 20(OH)D(2) does not require its transformation to 1,20(OH)(2)D(2) for its biological activity. Thus 20(OH)D(2) shows cell-type dependent antiproliferative and prodifferentiation activities through activation of VDR, while having no detectable toxic calcemic activity, and is a poor substrate for CYP27B1.”
https://pubmed.ncbi.nlm.nih.gov/21160030/
“1,24(S)-dihydroxyvitamin D2, an endogenous vitamin D2 metabolite, inhibits growth of breast cancer cells and tumors.”
Background: 1,24-Dihydroxyvitamin D2 (1,24(OH)2D2) is a naturally occurring metabolite of vitamin D2 with low calcemic activity and potent antiproliferative activity. We evaluated the activity of 1,24(OH)2D2 in breast cancer models.
Materials and methods: The antiproliferative activity of 1,24(OH)2D2 was quantitated against human and murine breast cancer cell lines. The antitumor activity of 1,24(OH)2D2 was quantitated using MCF-7 xenografts in nude mice.
Results: 1,24(OH)2D2 inhibited growth of vitamin D receptor (VDR)-positive, but not VDR-negative, breast cancer cells. 1,24(OH)2D2 (10 microg/kg or 50 microg/kg) reduced MCF-7 xenograft growth by 50% after five weeks. Tumor morphology in treated animals was consistent with replacement of epithelial cells by stromal tissue. Mice treated with 1,24(OH)2D2 showed no loss of body weight, hypercalcemia or kidney calcification.
Conclusion: 1,24(OH)2D2 inhibits growth of breast cancer cells via VDR-dependent mechanisms; its complete lack of toxicity and significant antitumor activity supports further development for chemotherapeutic applications.”
https://pubmed.ncbi.nlm.nih.gov/15816543/
Lumisterol molecules. Paradigm shift. A group like Grassroots isn’t going to recognize ANOTHER PATHWAY let alone a different family of receptors. Come back to reality folks.
There’s Lumisterol3 (L3), 20(OH)L3, 22(OH)L3,20,22(OH)2D3, pregnalumisterol (pL) to name a few. Below you see they are involved with the RoR’s. Master control.
Abstract
Using LC/qTOF-MS we detected lumisterol, 20-hydroxylumisterol, 22-hydroxylumisterol, 24-hydroxylumisterol, 20,22-dihydroxylumisterol, pregnalumisterol, 17-hydroxypregnalumisterol and 17,20-dihydroxypregnalumisterol in human serum and epidermis, and the porcine adrenal gland. The hydroxylumisterols inhibited proliferation of human skin cells in a cell type-dependent fashion with predominant effects on epidermal keratinocytes. They also inhibited melanoma proliferation in both monolayer and soft agar. 20-Hydroxylumisterol stimulated the expression of several genes, including those associated with keratinocyte differentiation and antioxidative responses, while inhibiting the expression of others including RORA and RORC. Molecular modeling and studies on VDRE-transcriptional activity excludes action through the genomic site of the VDR. However, their favorable interactions with the A-pocket in conjunction with VDR translocation studies suggest they may act on this non-genomic VDR site. Inhibition of RORα and RORγ transactivation activities in a Tet-on CHO cell reporter system, RORα co-activator assays and inhibition of (RORE)-LUC reporter activity in skin cells, in conjunction with molecular modeling, identified RORα and RORγ as excellent receptor candidates for the hydroxylumisterols. Thus, we have discovered a new biologically relevant, lumisterogenic pathway, the metabolites of which display biological activity. This opens a new area of endocrine research on the effects of the hydroxylumisterols on different pathways in different cells and the mechanisms involved.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5595834/
Most recently it was shown that both 20(OH)D3 and 20,23(OH)2D3 enhance defense mechanisms against UVB-induced oxidative stress and DNA damage in cultured human keratinocytes [23] and murine skin in vivo [22]. 20(OH)D3 and its hydroxymetabolites also show anti-cancer properties that are cell-lineage dependent [53, 54, 64, 68, 69, 88, 90, 92–97].
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5373926/
As ALWAYS, it’s what you don’t see. We won’t do any real investigation into how the association-based science is supposed to reduce disease burden. That would involve radio labeling molecules, tracking them, watching what they become, and seeing how they work. The pathogenesis model for the “Killing” of bad things you are to believe 25D ushers in. You know, the type of deep science that was done three, four, five, six DECADES AGO. Just to figure out the 25D and 1,25D. But today’s Scientists and Doctors are too busy with Cranial Rectal Inversion, or CRI, to accomplish anything.
Have a GREAT DAY!